Breaking Barriers in Antibody-Drug Conjugates Development
- Antibody-drug conjugates (ADCs) are an emerging class of targeted cancer therapies that combine potent cytotoxic drugs with tumor-specific antibodies. This approach promises to destroy cancer cells while sparing healthy tissue, offering a more precise alternative to traditional chemotherapy.
- ADC development has accelerated in recent years, leading to multiple regulatory approvals and a pipeline of new candidates in clinical trials. Despite this progress, significant challenges persist in ADC design, manufacturing, and analysis.
Antibody-Drug Conjugates Basics
Antibody-drug conjugates are complex biopharmaceuticals engineered to selectively deliver drugs to cancer cells. An ADC typically consists of a monoclonal antibody linked to a highly potent therapeutic payload (often a cytotoxic drug) via a specialized chemical linker. The antibody serves as a homing device, binding to a specific antigen abundantly expressed on cancer cells. Once the ADC binds to its target on a tumor cell, it is internalized and the cytotoxic drug is released inside the cell to induce cancer cell death. By concentrating the drug’s action at the tumor site, ADCs aim to maximize cancer cell killing while minimizing systemic side effects.

Each component of an ADC plays a crucial role in its therapeutic effect. The monoclonal antibody provides high specificity, recognizing and attaching to antigens mostly found on cancer cells and not on healthy cells. The linker that connects the drug to the antibody must be stable in the bloodstream to prevent premature release of the toxin, yet cleavable or triggerable within the target cell environment. The payload itself is a cytotoxic agent chosen for its extreme potency – far more potent than standard chemotherapy drugs to ensure that once delivered into a cancer cell, it can effectively kill the cell even at low concentrations. The design of an ADC is therefore a delicate balancing act: the antibody, linker, and payload must work in concert to achieve potent, tumor-specific activity without unacceptable toxicity.
Key Steps in ADC Development
ADC development is inherently multidisciplinary, requiring coordinated expertise in biologics, chemistry, and pharmacology. The process begins with selecting an appropriate target antigen. That antigen should strongly expressed on cancer cells but minimally present on normal cells. Researchers then generate a high-affinity monoclonal antibody against this target, often using advanced discovery platforms to ensure specificity and reduced immunogenicity. With a targeting antibody in hand, a compatible cytotoxic payload is chosen. The payload must be exceptionally potent and ideally suited to the tumor type.1 A suitable linker is designed to attach the payload to the antibody; this linker must remain intact during the ADC’s journey through the bloodstream and then release the drug under defined conditions inside the tumor cell. Early in development, researchers often test a few different linker-payload combinations to find the optimal balance of stability and efficacy.
Once an ADC candidate is constructed, extensive characterization and optimization are undertaken. ADC process development involves refining the conjugation chemistry and production methods to reliably generate the ADC at larger scales without losing its activity. Adjustments may be made to control the drug-to-antibody ratio (DAR) – the average number of drug molecules attached to each antibody. An appropriate DAR is critical for efficacy and safety. If too few payload molecules are attached, the ADC may be less effective; too many can destabilize the antibody or increase toxicity.2 Process engineers also work to ensure that the conjugation reaction yields a consistent product with minimal aggregates or free (unconjugated) drug impurities, since these can impact safety profiles. Throughout this stage, small-scale pilot batches of the ADC are produced and analyzed to fine-tune reaction conditions, purification steps, and storage formulations.

Preclinical testing is another key step in ADC development. The optimized ADC is evaluated in cellular assays to confirm it binds the target antigen and kills the antigen-expressing cells. It is also tested in animal models of cancer to assess tumor targeting and therapeutic efficacy, as well as to observe any toxic effects on normal tissues. These studies help determine a safe and active dose range to carry forward.
Notably, ADC development often requires specialized models. If a target antigen is human-specific, developers might use tumor xenograft models or transgenic animals to ensure the antibody can bind in vivo. Meanwhile, developers must also address pharmacokinetics (how the ADC distributes and clears in the body) and potential immunogenicity (whether the immune system might react against the ADC).
Crucially, many organizations choose to partner with specialized contract development and manufacturing organizations (CDMOs) to navigate these steps. Biologic drugs production and conjugation them with a cytotoxic payloads is a combination of capabilities that not all companies have in-house. Indeed, the growing popularity of ADCs has driven increased collaboration between firms with antibody expertise and those with small-molecule or conjugation expertise.
Mabion Biologics CDMO with dedicated ADC services can provide end-to-end support under one roof. Engaging CDMO early even at the preclinical stage can accelerate progress. By the time an ADC is ready to enter clinical trials, a robust manufacturing process and a thorough understanding of its critical quality attributes should be in place, setting the stage for the next development phases.
Challenges in ADC Design, Linker Stability, and Payload Selection
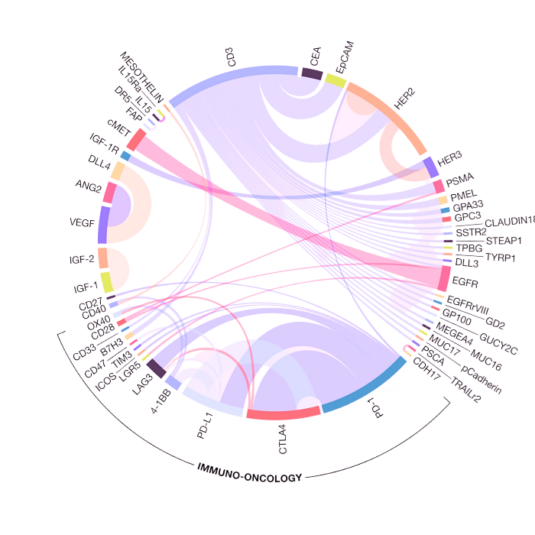
Designing a successful ADC is a complex endeavor, with multiple interdependent challenges. One fundamental consideration is selecting the right target antigen and antibody. The ideal target for an ADC is one that is highly expressed on cancer cells but absent (or at very low levels) on normal cells. If the target is also present on healthy tissues, the ADC may attack those cells as well, leading to off-target toxicity. Even when a suitable target is identified, tumors can be heterogeneous. Not every cell in a tumor expresses the target antigen at the same level or at all. This heterogeneity can cause some cancer cells to escape the ADC, which in turn can lead to treatment resistance.

To address this, researchers carefully evaluate target expression patterns and sometimes design antibodies that bind to multiple epitopes or multiple targets on tumor cells. The antibody itself must also be optimized: it should bind strongly to the target and internalize efficiently, and it should be engineered (often humanized or fully human) to avoid immune rejection by the patient.4
Another critical challenge lies in linker stability. The linker is the molecular tether that attaches the payload to the antibody, and its behavior can make or break an ADC’s safety and efficacy. In the bloodstream, the linker must be extraordinarily stable – it should not release the toxic payload prematurely, or the drug would harm healthy cells before reaching the tumor. At the same time, once the ADC is inside a cancer cell (typically in an endosome or lysosome after internalization), the linker needs to release the payload effectively. Developers have designed both cleavable linkers and non-cleavable linkers to achieve this controlled release.5 Cleavable linkers are engineered to break under specific conditions found inside cells, such as the presence of certain enzymes or the acidic pH in lysosomes. For example, some linkers include peptide sequences that are cut by proteases abundant in tumors, while others break in low pH or high glutathione environments. Non-cleavable linkers, by contrast, do not break chemically; instead, the entire ADC is degraded inside the cell, and the payload is released as part of the breakdown of the antibody. Each approach has pros and cons: cleavable linkers can efficiently release drug inside target cells but carry a slight risk of instability if similar conditions are present in circulation, whereas non-cleavable linkers offer exceptional stability in the bloodstream but rely on complete antibody degradation to deploy the drug. Achieving the right balance – a linker stable enough to travel through the body, yet adequately triggered in the tumor – is often a major hurdle in ADC design. Indeed, linker stability issues were a problem in some early ADC candidates, leading to toxicity or insufficient potency, and overcoming this required significant chemical innovation.6

Payload selection is the third major design challenge. The payload drugs used in ADCs are generally far more potent than standard chemotherapy agents. They need to be, because only a small amount of drug is delivered to each cancer cell by the antibody. Classic payloads in approved ADCs include microtubule-disrupting agents (like auristatins and maytansinoids) and DNA-damaging agents (like calicheamicin or pyrrolobenzodiazepine dimer). These molecules can kill cells at picomolar concentrations.7 However, different payloads have different strengths and limitations. For example, auristatins (such as MMAE) are very potent but can diffuse out of target cells (a “bystander effect” that can be useful against neighboring tumor cells, but risky if neighboring healthy cells are present). DNA cross-linkers are extremely toxic but may have trouble penetrating large solid tumors.8 Moreover, some payloads that worked well in blood cancers proved less effective in solid tumors, partly due to differences in how well the ADC is internalized or how the payload acts in the tumor microenvironment.9

As a result, selecting the right payload for a given target and cancer type is a nuanced decision. Linker-payload compatibility is also an issue – the chemistry of the linker and the drug must be compatible so that the conjugation is stable and the drug can be released properly inside the cell. New payload classes are now being explored to expand what ADCs can do. For instance, topoisomerase I inhibitors have been introduced as ADC payloads to tackle cancers that didn’t respond as well to earlier payloads; this class of drugs (exemplified by deruxtecan in some recent ADCs) can be very effective against solid tumors.10 Other innovative payload concepts include immune stimulators (to rally an immune attack on the tumor when the ADC arrives) and even agents that target intracellular signaling or protein machinery (such as payloads that induce targeted protein degradation).9 With each potential payload, developers must consider potency, mechanism of action, and how well the tumor cells can be killed without the drug leaking to healthy cells.
Payload selection and linker stability are tightly linked design concerns. The optimal pairing of a payload with a suitable linker and antibody often requires extensive experimentation and fine-tuning.
Analytical and Quality Control Considerations in ADC Development
Antibody-drug conjugates are among the most analytically complex therapeutics to develop. Each ADC is essentially a combination of a large biologic (the antibody) and a small-molecule drug, and this dual nature means that analytical and quality control teams must characterize both components as well as the conjugated product. Regulatory authorities expect a thorough understanding of an ADC’s quality attributes, which in practice requires a battery of advanced analytical methods. Early in development and certainly by the time of clinical trials, ADC development teams need to answer questions such as:
- What is the drug-to-antibody ratio and distribution?
- How pure is the ADC (are there antibody aggregates or free drug present)?
- Does the antibody still bind to the target antigen after conjugation?
- How stable is the ADC in serum (does it lose the payload over time)?
- Which analytical techniques for characterizing ADCs at different stages of development can be performed in-house, and which require outsourcing?
Fundamental parameter of ADC characterization is the drug-to-antibody ratio. DAR affects potency and safety. A low DAR might reduce efficacy, while a very high DAR can impair the antibody’s structure or cause rapid clearance and toxicity. To measure DAR and the distribution of different ADC species, methods like mass spectrometry (MS) and high-performance liquid chromatography (HPLC) are widely used. Hydrophobic interaction chromatography (HIC) can separate ADC molecules based on how many drugs are attached, revealing the distribution of DAR species. Mass spectrometry, often coupled with liquid chromatography (LC-MS), provides detailed insights into both the average DAR and the exact attachment sites on the antibody. Importantly, modern LC-MS methods are sensitive enough to detect even small amounts of free payload or to characterize third-generation ADCs with very potent drugs at low concentrations. These techniques help ensure that each batch of ADC has the intended composition and that any deviations can be caught early.2
Another critical set of assays are those assessing the biological activity of the ADC. A ligand-binding assay (LBA), for instance, can confirm that the ADC’s antibody portion still binds to the target antigen correctly. LBAs can also be used to measure how much of the antibody in a sample is conjugated versus unconjugated, by using capture reagents specific to the payload or the antibody.11
Cell-based assays play a central role in confirming that ADCs retain their cytotoxic efficacy after conjugation. These assays allow researchers to directly observe the interaction of ADCs with live cells expressing target antigens, providing functional validation of the therapeutic’s design, potency, and mode of action.12 Cytotoxicity assays are among the most widely used cell-based methods to assess ADC potency. These assays expose antigen-positive tumor cell lines to a range of ADC concentrations, quantifying cell death to determine the inhibitory concentration (IC₅₀). An IC₅₀ value of ~10 nM or lower is generally considered indicative of a potent ADC candidate.
Another critical functional endpoint is internalization. The antibody internalization assay measures how efficiently the ADC is taken up by target cells following antigen binding. Internalization is necessary for the payload to be released inside the cell and execute its cytotoxic function.
Cell-based studies also enable deeper analysis of the mechanism of action by examining the downstream effects of internalized payloads. Apoptosis assays, such as caspase-3/7 activation and Annexin V-based phosphatidylserine exposure, reveal whether the ADC induces programmed cell death.13 These endpoints are commonly used in tandem with proliferation assays to generate a complete view of ADC efficacy. Mabion’s validated platforms ensure these critical apoptotic markers are detected with high sensitivity and reproducibility.
Receptor density studies further refine ADC suitability. By quantifying antigen copies per cell, these assays determine whether a target is sufficiently expressed for effective ADC binding and internalization. A threshold of approximately 10,000 receptors per cell is often cited as necessary for consistent therapeutic action.
Additionally, stability studies are performed by incubating the ADC in human serum or plasma and measuring whether the payload remains attached over time or if any degradation products appear. Quality control of ADCs must also address the payload’s potency: the manufacturing process should consistently achieve the correct dosage of toxin per antibody, and ensure batch-to-batch consistency.
Landscape for Antibody-Drug Conjugates
The landscape for antibody-drug conjugates has evolved from a niche experimental idea into one of the most dynamic areas of oncology therapeutics. ADCs are now regarded as one of the fastest-growing segments in oncology drug development, thanks in large part to a string of clinical successes in recent years. There are over a dozen ADCs approved for cancer treatment worldwide and nearly 100 new ADC candidates are in clinical trials as of the mid-2020s.14

This surge is driven by the promise ADCs have shown in delivering meaningful benefits to patients, even in cancers that were refractory to standard treatments. High-profile examples, such as HER2-targeting ADCs for breast cancer, have demonstrated that ADCs can achieve potent tumor control with manageable toxicity, validating the approach and attracting investment from both large pharmaceutical companies and biotech startups.15
In this booming landscape, partnerships and collaborations are central. Developing an ADC requires integrating skills in biologics and chemistry, and many organizations choose to collaborate to combine these strengths. We have seen numerous partnerships where a company with a novel antibody teams up with another that has a potent payload or linker technology.
Big pharma companies have also made strategic acquisitions of ADC-focused biotech companies to bring promising ADC candidates and expertise in-house. Moreover, nearly every major oncology company from global TOP30 list now has an ADC program or is licensing ADC technology, underscoring how integral this modality has become to the future of cancer therapy.
New Approaches Transforming ADC Development
The landscape of ADC development is undergoing a structural transformation. At the center of this shift are organizations like Mabion, embracing a co-development-driven model tailored for speed, flexibility, and scientific depth. Mabion’s strategy highlights a targeted commitment to becoming a preferred CDMO and co-developer for ADCs, particularly in the biological drug substance segment.
Mabion’s strength lies in its established foundation in biologics development. As a GMP-certified biologics CDMO, the company offers robust scientific infrastructure and deep technical capabilities in antibody design, expression, and analytical characterization. Our expansion into the ADC space reflects an evolution toward delivering integrated bioconjugate solutions. Initially focused on partnering for biologics development and manufacturing, Mabion is actively building the expertise and facilities required to bring conjugation technologies in-house by 2026. This positions the company as a reliable partner in ADC development from antibody engineering to payload integration and analytics.

Mabion’s approach centers on mastering the biological component — producing high-quality, scalable antibodies optimized for conjugation efficiency, internalization, and specificity. This focus is essential as modern ADCs increasingly depend on tailored bioconjugation strategies and advanced targeting frameworks.
Key to Mabion’s model is their emphasis on co-development. Rather than functioning solely as a service provider, Mabion aims to partner earlier in the development process, sharing both risk and innovation. Through these partnerships, Mabion helps clients address payload selection, antigen targeting strategies, and preclinical readiness. Our integrated analytics platform supports rapid antibody screening, functional characterization, and developability assessments. As ADCs move beyond traditional cytotoxins toward novel payloads conjugation chemistries becomes more nuanced.16 Our ambition to internalize conjugation capabilities reflects our intent to manage this complexity directly. Doing so would allow us to better control all vital parameters in ensuring ADC safety and efficacy.
Conclusion
The ADC field is breaking barriers on multiple fronts. Site-specific conjugation technologies are yielding cleaner, safer products. New linkers and payloads are expanding the range of cancers that ADCs can effectively treat. A deeper biological insight into how tumors respond to ADCs is guiding smarter designs and combination strategies. On top of that, the practical know-how of making ADCs is improving, which lowers some of the historic hurdles in development. For decision-makers and scientists in the biopharma industry, these developments signal that ADCs are entering a renaissance.
The lessons learned from earlier challenges have given rise to innovative solutions, transforming ADC development from a high-risk venture into a more predictable and fertile ground for cancer drug development.
With partners like Mabion offering co-development and cutting-edge expertise, even companies new to ADCs can confidently explore this promising modality. The coming years are likely to bring a new wave of ADC therapies that are more potent, more tumor-selective, and more patient-friendly than ever before, truly realizing the vision of the “magic bullet” in cancer treatment.
FAQ
Prepared by:

Marketing Specialist
References
- Wang Z, Li H, Gou L, Li W, Wang Y. Antibody-drug conjugates: Recent advances in payloads. Acta Pharm Sin B. 2023; 13(10): 4025-4059.
- Matsuda Y, Mendelsohn BA. Recent Advances in Drug-Antibody Ratio Determination of Antibody-Drug Conjugates. Chem Pharm Bull (Tokyo). 2021; 69(10): 976-983.
- Marei HE, Cenciarelli C, Hasan A. Potential of antibody–drug conjugates (ADCs) for cancer therapy. Cancer Cell Int. 2022; 22: 255.
- Drago JZ, Modi S, Chandarlapaty S. Unlocking the potential of antibody-drug conjugates for cancer therapy. Nat Rev Clin Oncol. 2021; 18(6): 327-344.
- Lei Y, Zheng M, Chen P, Seng Ng C, Peng Loh T, Liu H. Linker Design for the Antibody Drug Conjugates: A Comprehensive Review. ChemMedChem. 2025; 20(15): e202500262.
- Su Z, Xiao D, Xie F, Liu L, Wang Y, Fan S, Zhou X, Li S. Antibody-drug conjugates: Recent advances in linker chemistry. Acta Pharm Sin B. 2021; 11(12): 3889-3907.
- Lin C, Hadfield MJ, Santopietro A, Lagos G, Cheng L, El-Deiry WS, Aggarwal R, Mega A, Hyams E, Carneiro BA. The evolving landscape of antibody-drug conjugates (ADCs) for treatment of prostate cancer. NPJ Precis Oncol. 2025; 9(1): 351.
- Miller ML, Shizuka M, Wilhelm A, Salomon P, Reid EE, Lanieri L, Sikka S, Maloney EK, Harvey L, Qiu Q, Archer KE, Bai C, Vitharana D, Harris L, Singh R, Ponte JF, Yoder NC, Kovtun Y, Lai KC, Ab O, Pinkas J, Keating TA, Chari RVJ. A DNA-Interacting Payload Designed to Eliminate Cross-Linking Improves the Therapeutic Index of Antibody-Drug Conjugates (ADCs). Mol Cancer Ther. 2018; 17(3): 650-660.
- Izzo D, Ascione L, Guidi L, Marsicano RM, Koukoutzeli C, Trapani D, Curigliano G. Innovative payloads for ADCs in cancer treatment: moving beyond the selective delivery of chemotherapy. Ther Adv Med Oncol. 2025; 17: 17588359241309461.
- Pommier Y, Thomas A. New Life of Topoisomerase I Inhibitors as Antibody-Drug Conjugate Warheads. Clin Cancer Res. 2023; 29(6): 991-993.
- Hou Y, Miao J, Sun Y, Shi L, Ouyang L, Chen X, Li Z, Liu T, Qin G, Qin Q, Gong L. Ligand-binding assays validated for quantitative bioanalysis of a novel antibody-drug conjugate in monkey serum and related application in a nonclinical study. J Pharmacol Toxicol Methods. 2025; 131: 107580.
- Xu W, Bano N, Guzman-Valdes O, Amberman J, Bandlamudi E, Khanna P, Carmean R, Helmy R. Development and Validation of a Cell-Based Binding Neutralizing Antibody Assay for an Antibody-Drug Conjugate. AAPS J. 2024; 26(3): 37.
- Moldovan C, Onaciu A, Toma V, Munteanu RA, Gulei D, Moldovan AI, Stiufiuc GF, Feder RI, Cenariu D, Iuga CA, Stiufiuc RI. Current trends in luminescence-based assessment of apoptosis. RSC Adv. 2023; 13(45): 31641-31658.
- Chen B, Zheng X, Wu J, Chen G, Yu J, Xu Y, Wu WKK, Tse GMK, To KF, Kang W. Antibody-drug conjugates in cancer therapy: current landscape, challenges, and future directions. Mol Cancer. 2025; 24(1): 279.
- Ma H, Li J. Impact of HER2-targeting antibody drug conjugates in treatment strategies for patients with breast cancer. Heliyon. 2025; 11(3): e41590.
- Kostova V, Désos P, Starck JB, Kotschy A. The Chemistry Behind ADCs. Pharmaceuticals (Basel). 2021; 14(5): 442.