Oncologic Bispecific Antibodies in Immunotherapy
- Oncologic bispecific antibodies are reshaping immunotherapy by enabling mechanisms beyond conventional monoclonal antibodies. Their success depends on the right target pair, the right molecular format, and the right development strategy.
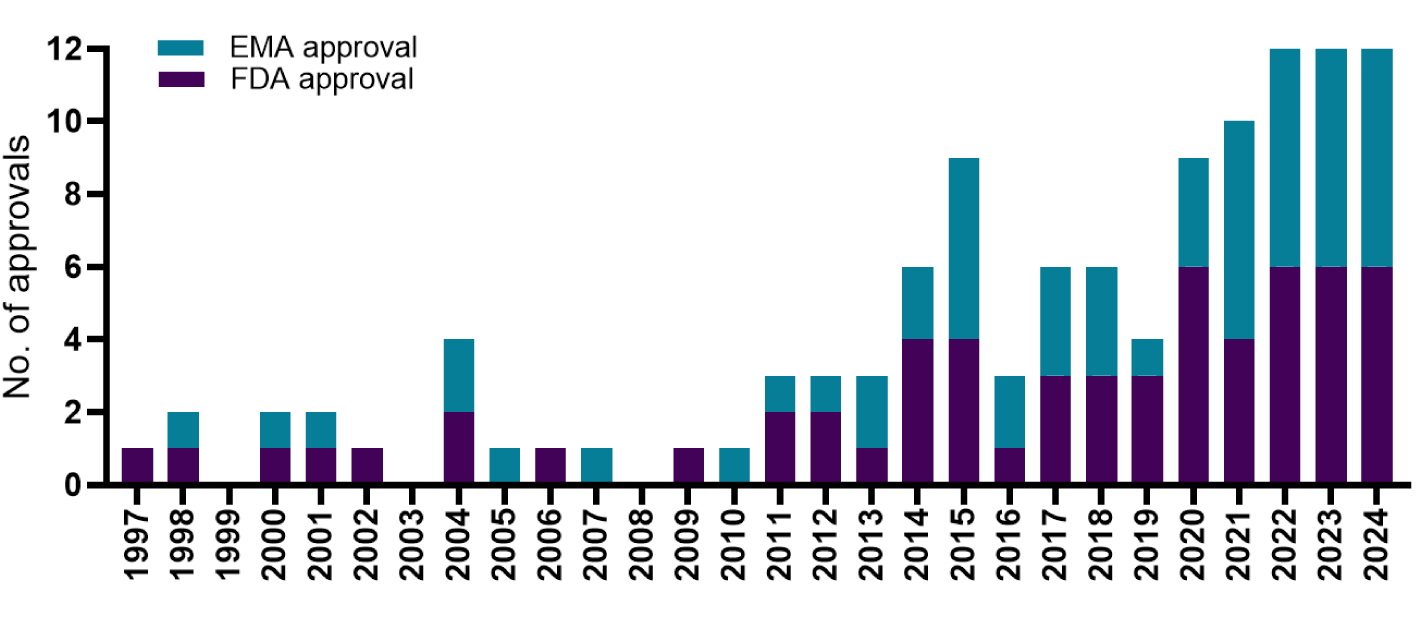
- Clinical progress has accelerated rapidly, with numerous regulatory approvals since 2014 for both hematologic malignancies and solid tumors. The success of bispecific antibodies is closely linked to target biology.
- Strategic challenge for biotech companies developing bispecific antibodies is translation from therapeutic concept to manufacturing.
How do Bispecific Antibodies Work?
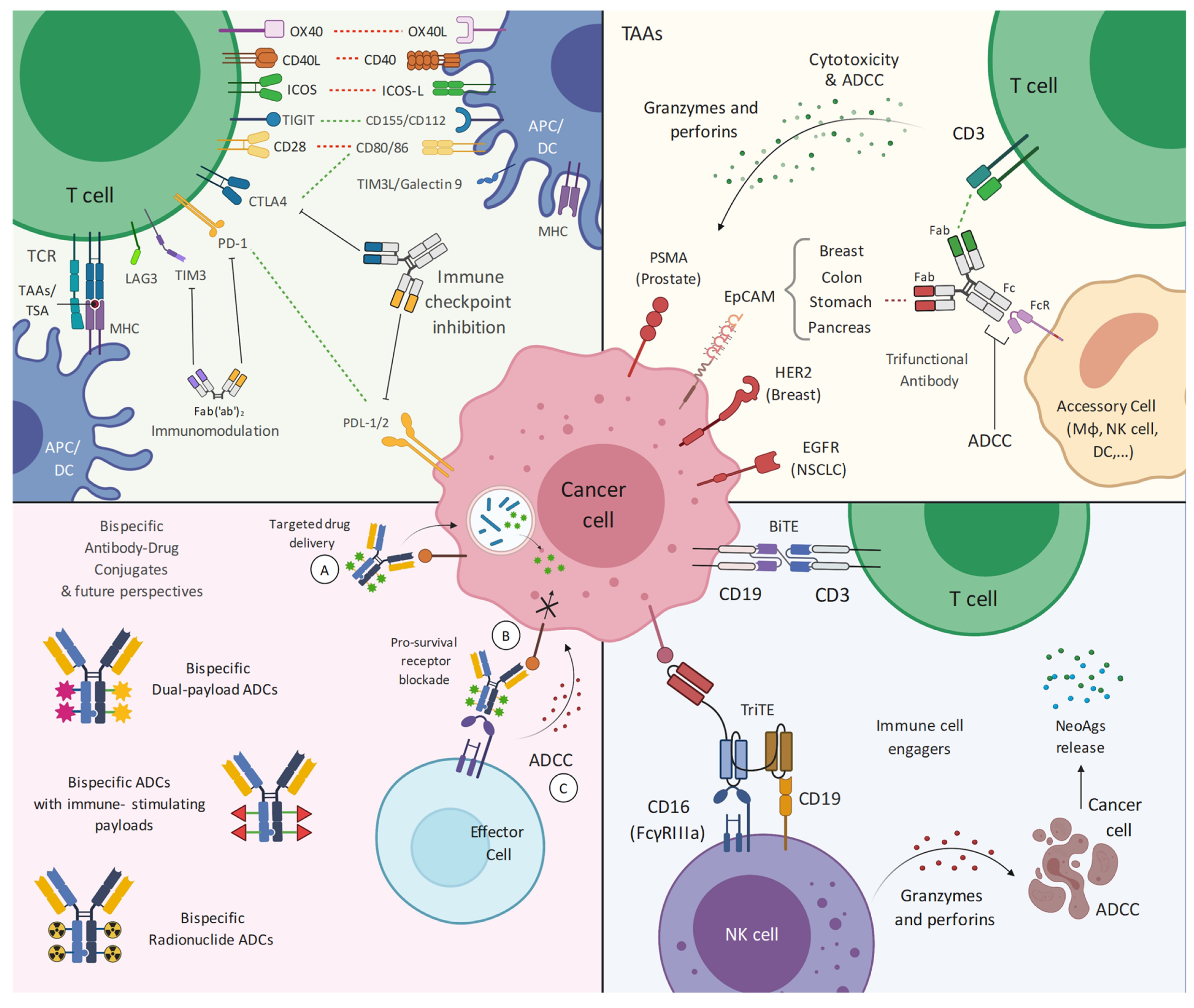
Bispecific antibodies (bsAbs) are biologics designed to bind two different molecular targets or two distinct epitopes on the same target. In oncology, this dual-binding capacity enables therapeutic mechanisms that are difficult or impossible to achieve with conventional monoclonal antibodies. Structurally, bispecific antibodies can be designed as fragment-based molecules, IgG-like antibodies, Fc-containing formats, Fc-silenced constructs, biparatopic antibodies, or fusion proteins.
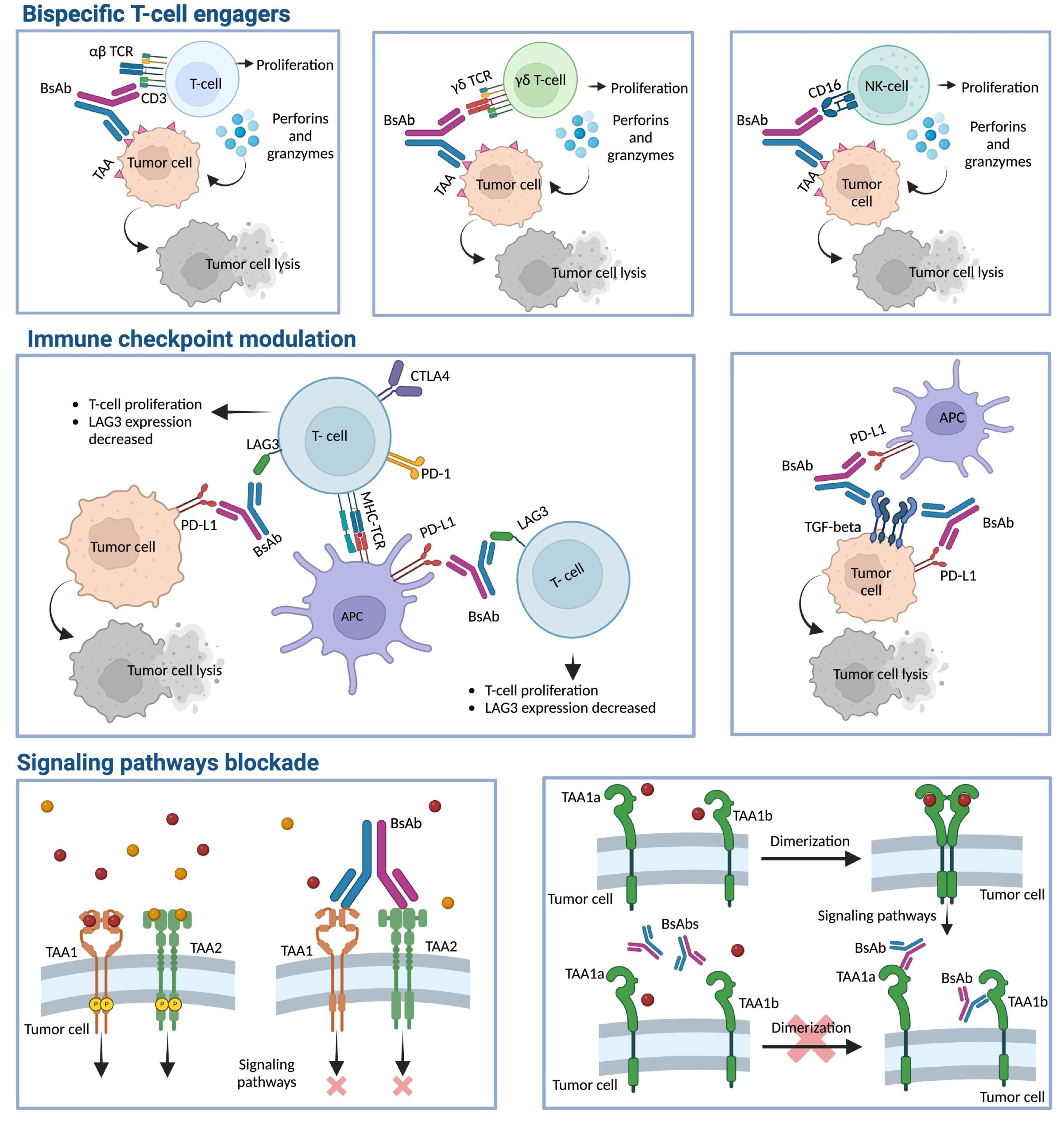
The best-known mechanism in oncology is immune-cell redirection. In this approach, one binding arm recognizes a tumor-associated antigen, while the second arm binds an immune-effector receptor, most commonly CD3 on T cells. By physically bringing a cytotoxic T cell into close proximity with a malignant cell, the bispecific antibody promotes immune synapse formation, T-cell activation, release of cytotoxic granules, and tumor-cell killing. Importantly, this mechanism can bypass the need for conventional antigen presentation by major histocompatibility complex molecules, which is one reason why CD3-engaging bsAbs have become such an important class in hematologic malignancies.2
Not all oncologic bispecific antibodies function by T-cell engagement. Some are designed to inhibit two signaling pathways at the same time, for example by targeting receptors involved in tumor growth, survival, invasion, or resistance to therapy. Others bind two epitopes on the same receptor, increasing avidity, promoting receptor clustering, or enhancing internalization. Checkpoint-directed bispecifics aim to modulate immune suppression in the tumor microenvironment. Peptide-HLA-directed molecules expand the target space toward intracellular tumor antigens presented on the cell surface.3
Because the mechanism of action is embedded in the molecule’s architecture, bispecific antibody development must consider biology and chemistry, manufacturing, and controls in parallel. Binding geometry, affinity, valency, linker design, glycosylation, aggregation propensity, stability, and chain-pairing fidelity can all influence therapeutic activity and product quality.
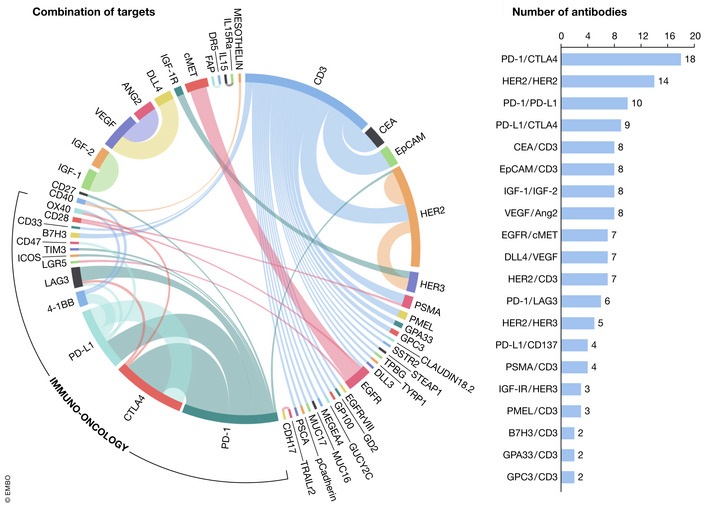
Popular Targets for Oncologic Bispecific Antibodies
Target selection is one of the most important strategic decisions in oncologic bispecific antibody development. Clinically meaningful target pair should support a sufficient antigen density and adequate tumor selectivity.
CD3
CD3 is the most established immune-effector target in oncologic bispecific antibodies. It is part of the T-cell receptor complex and is required for T-cell activation. CD3-binding bispecific antibodies do not target CD3-positive cells for destruction. These agents connect native T lymphocytes with tumor cells by simultaneously binding CD3 and a specific tumor-associated antigen. This mechanism has been clinically validated across several hematologic malignancies and is now being extended into selected solid tumor settings.5 Bispecific antibodies targeting CD3 include:
- Blinatumomab (CD19 × CD3) for B-cell precursor acute lymphoblastic leukemia (ALL).
- Mosunetuzumab (CD20 × CD3) for relapsed or refractory follicular lymphoma (FL).
- Epcoritamab (CD20 × CD3) for relapsed or refractory FL or diffuse large B-cell lymphoma (DLBCL).
- Glofitamab (CD20 × CD3) for relapsed or refractory DLBCL or large B-cell lymphoma arising from follicular lymphoma.
- Odronextamab (CD20 × CD3) for relapsed or refractory FL or DLBCL.
- Talquetamab (GPRC5D × CD3) for refractory multiple myeloma (MM).
- Teclistamab (BCMA × CD3) for refractory MM.
- Elranatamab (BCMA × CD3) for refractory MM.
- Linvoseltamab (BCMA × CD3) for refractory MM.
- Tarlatamab (DLL3 × CD3) for extensive-stage small cell lung cancer (SCLC).
- Catumaxomab (EpCAM × CD3) for malignant ascites in EpCAM-positive tumors.
- Tebentafusp (gp100 × CD3) for unresectable or metastatic uveal melanoma.
These therapies effectively weaponize a patient’s own T-cells to mount a potent, targeted attack against malignant cells. Despite their power, CD3-targeting therapies are associated with unique and potentially life-threatening toxicities. Widespread T-cell activation can lead to cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS). Clinical management of these side effects often involves step-up dosing regimens and prophylactic treatments to mitigate the peak levels of inflammatory cytokines. Recent innovations, such as subcutaneous administration, have also shown potential in reducing the severity of CRS compared to traditional intravenous routes.6
Research continues to optimize CD3 binding to enhance the therapeutic window of these agents. Tuning the affinity of the CD3-binding arm is a critical strategy. Lower-affinity antibodies can sometimes kill tumor cells more effectively while reducing the risk of excessive cytokine release.
ErbB family
The ErbB receptor tyrosine kinase (RTK) family, which includes EGFR, HER2, and HER3, represents a critical set of targets for solid tumor oncology. These receptors are frequently overexpressed or mutated in various epithelial tumors, including those of the lung, breast, and gastrointestinal tract. The ErbB family is attractive as a target for bispecific antibodies because it allows mechanisms beyond immune cell redirection. Bispecific antibodies targeting EGFR, HER2 or HER3 include:
- Amivantamab (EGFR × MET) for non-small cell lung cancer (NSCLC).
- Zanidatamab (HER2 × HER2) for biliary tract cancer (BTC).
- Zenocutuzumab (HER2 × HER3) for NSCLC, BTC, and pancreatic adenocarcinoma.
Immune checkpoints
Immune checkpoints regulate T-cell activation and help maintain immune homeostasis. In cancer, these pathways can be exploited by tumors to suppress antitumor immunity. Checkpoint-focused bispecific antibody development requires a different analytical mindset from cytotoxic T-cell engagers.
Dual checkpoint bsAbs are designed to inhibit two suppressive pathways with one molecule. For example, PD-1 × CTLA-4 drug aim to broaden immune activation while potentially altering tissue distribution, avidity, or pharmacokinetic behavior compared with administering two separate antibodies. Other approaches combine checkpoint blockade with additional tumor microenvironment modulation, such as PD-L1 × TGF-β pathway targeting, to address both T-cell inhibition and stromal or immunosuppressive barriers.
A particularly important design direction is conditional immune costimulation. Bispecifics can be designed to activate costimulatory signaling preferentially in PD-L1-positive tumor environments. The goal is to avoid broad systemic activation of costimulatory receptors while enhancing T-cell function where tumor-associated immune suppression is present.
Approved Bispecific Antibodies in Cancer Immunotherapy
The clinical approval of bispecific antibodies in oncology reflects decades of technological progress in antibody engineering. Early bispecific formats demonstrated that two binding specificities could be combined within a single therapeutic molecule, but they also exposed important process development challenges, including:
- Short half-life
- Complex administration
- Manufacturing constraints
- Need for precise control of immune activation
As the field matured, bispecific antibody technology evolved from relatively simple T-cell-engaging constructs toward more sophisticated, manufacturable, and clinically flexible formats. Newer molecules increasingly incorporate Fc regions to extend serum half-life, improve developability, and support more convenient dosing schedules. At the same time, antibody engineering strategies have improved correct chain pairing, reduced unwanted species, optimized binding geometry, and enabled more controlled activation of immune effector cells.
The first major clinical validation of oncologic bispecific antibodies came from CD19 × CD3 T-cell engagement. Blinatumomab targets CD19 on B-lineage cells and CD3 on T cells and is used in CD19-positive B-cell precursor acute lymphoblastic leukemia. Its approval established T-cell redirection as a clinically viable mechanism and demonstrated that a bispecific format could convert endogenous T cells into targeted cytotoxic effectors.
The timeline of FDA-approved bispecific antibodies began in 2014 with blinatumomab, marking a significant milestone in targeted therapy. Initially approved for Philadelphia chromosome-negative relapsed or refractory B-cell precursor ALL.8
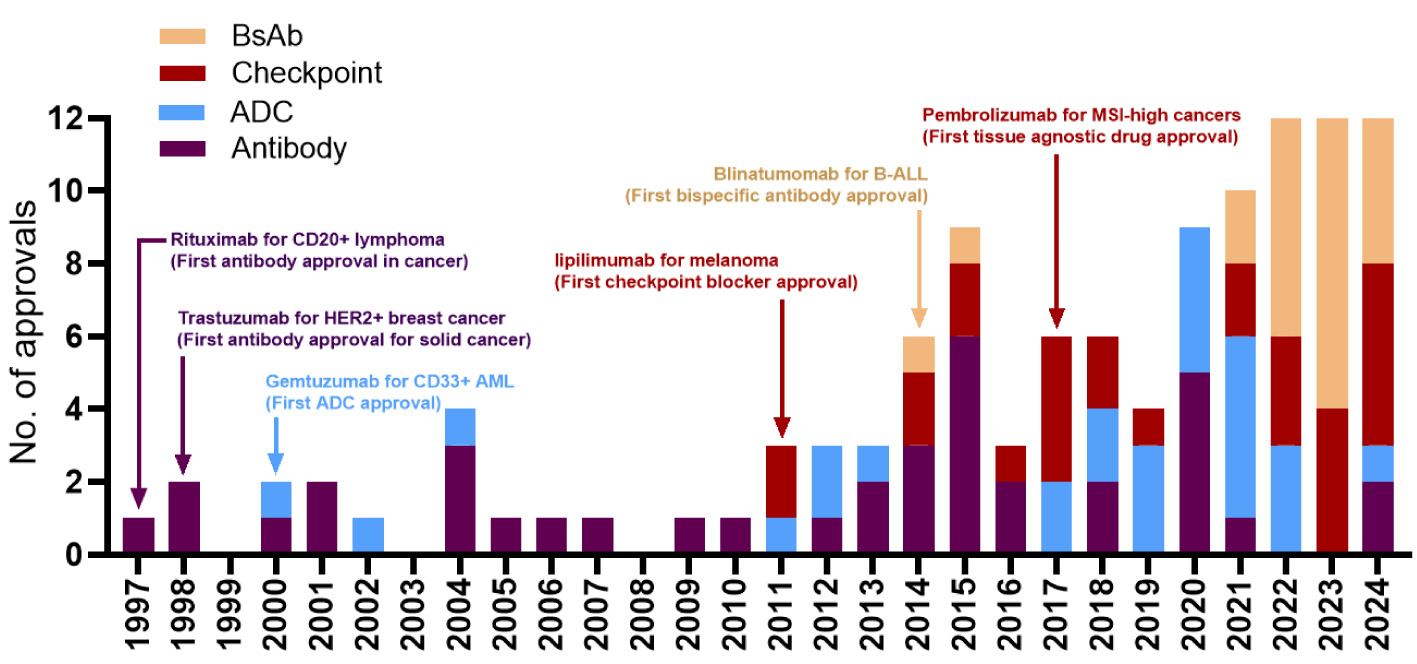
More recent approvals in solid tumors show that bispecific antibody technology is expanding beyond classical immune-cell redirection. The recent success of approved agents reflects a shift from simple format to multivalent configurations that enhance binding avidity to tumor antigens. Technological breakthroughs have also enabled biparatopic binding, where a single molecule targets two non-overlapping epitopes on the same receptor to more effectively block compensatory growth signals.9
Future Perspectives of Oncologic Bispecific Antibodies
The future of oncologic bsAbs lies in the expansion toward next-generation and multispecific formats:
- NK-cell engagers
- Myeloid-cell engagers
- Masked bispecific antibodies
- Conditionally activated molecules
- Trispecific antibodies
- Bispecific antibody-drug conjugates
Advanced constructs aim for even greater precision by targeting three or more antigens simultaneously, which can further curtail resistance and enhance immune cell recruitment. These technologies may help address limitations of current T-cell engagers.
For example, bispecific antibody-drug conjugates (BsADCs) are being investigated. These molecules combine the precise targeting of a bsAbs with the potent cytotoxic power of a chemical payload, essentially creating a “pharmaceutical Trojan horse“.
The future of oncologic bispecific antibodies will likely be shaped by expansion into solid tumors. Strategies involve using biomarkers to predict responses and optimizing intratumoral delivery to bypass dense stromal barriers.
FAQ
Prepared by:

Marketing Specialist
References
- Herrera M, Pretelli G, Desai J, Garralda E, Siu LL, Steiner TM, Au L. Bispecific antibodies: advancing precision oncology. Trends Cancer. 2024; 10(10): 893-919.
- Guo X, Wu Y, Xue Y, Xie N, Shen G. Revolutionizing cancer immunotherapy: unleashing the potential of bispecific antibodies for targeted treatment. Front Immunol. 2023; 14: 1291836.
- Holland CJ, Crean RM, Pentier JM, de Wet B, Lloyd A, Srikannathasan V, Lissin N, Lloyd KA, Blicher TH, Conroy PJ, Hock M, Pengelly RJ, Spinner TE, Cameron B, Potter EA, Jeyanthan A, Molloy PE, Sami M, Aleksic M, Liddy N, Robinson RA, Harper S, Lepore M, Pudney CR, van der Kamp MW, Rizkallah PJ, Jakobsen BK, Vuidepot A, Cole DK. Specificity of bispecific T cell receptors and antibodies targeting peptide-HLA. J Clin Invest. 2020; 130(5): 2673-2688.
- Wang S, Chen K, Lei Q, Ma P, Yuan AQ, Zhao Y, Jiang Y, Fang H, Xing S, Fang Y, Jiang N, Miao H, Zhang M, Sun S, Yu Z, Tao W, Zhu Q, Nie Y, Li N. The state of the art of bispecific antibodies for treating human malignancies. EMBO Mol Med. 2021; 13(9): e14291.
- Kassner J, Abdellatif B, Yamshon S, Monge J, Kaner J. Current landscape of CD3 bispecific antibodies in hematologic malignancies. Trends Cancer. 2024; 10(8): 708-732.
- Lloyd K, Middelburg J, Ovcinnikovs V, Pencheva N, Kemper K, van Hall T. Improving CD3 bispecific antibody therapy in solid tumors using combination strategies. Front Oncol. 2025; 15: 1548446.
- Paul S, Zhou S. Six events that shaped antibody approvals in oncology. Front Immunol. 2025; 16: 1533796.
- Sanford M. Blinatumomab: first global approval. Drugs. 2015; 75(3): 321-327.
- Shui L, Wu D, Yang K, Sun C, Li Q, Yin R. Bispecific antibodies: unleashing a new era in oncology treatment. Mol Cancer. 2025; 24(1): 212.
- Antonarelli G, Giugliano F, Corti C, Repetto M, Tarantino P, Curigliano G. Research and Clinical Landscape of Bispecific Antibodies for the Treatment of Solid Malignancies. Pharmaceuticals (Basel). 2021; 14(9): 884.


